Glaucoma Kala Motia
Glaucoma kala motia is known as ‘the silent thief of sight’ because patients can loose their outer-most vision over time with no other symptoms. Due to the chronic nature of the disease sight is stolen bit by bit and by the time you realize it you may already have significant loss of vision.
There are more than 1.8 million glaucoma patients in Pakistan and almost half of them have already lost their eyesight permanently due to delay in diagnosis and treatment. In Pakistan 50% of people don’t even know they have the disease.
Many people believe that blindness is not preventable and just a part of normal ageing. Programs that target blindness and conditions that cause it, can change not only the lives of individuals but also the country as a whole. Visit your doctor for yearly screening for glaucoma from the age of 40 years.
What is glaucoma kala motia?
The glaucoma causes damage to your eye’s optic nerve. Increased pressure in your eye is caused by fluid that builds up in the front part of your eye. This pressure damages your optic nerve. Blindness from glaucoma can often be prevented with early treatment
Causes of glaucoma?
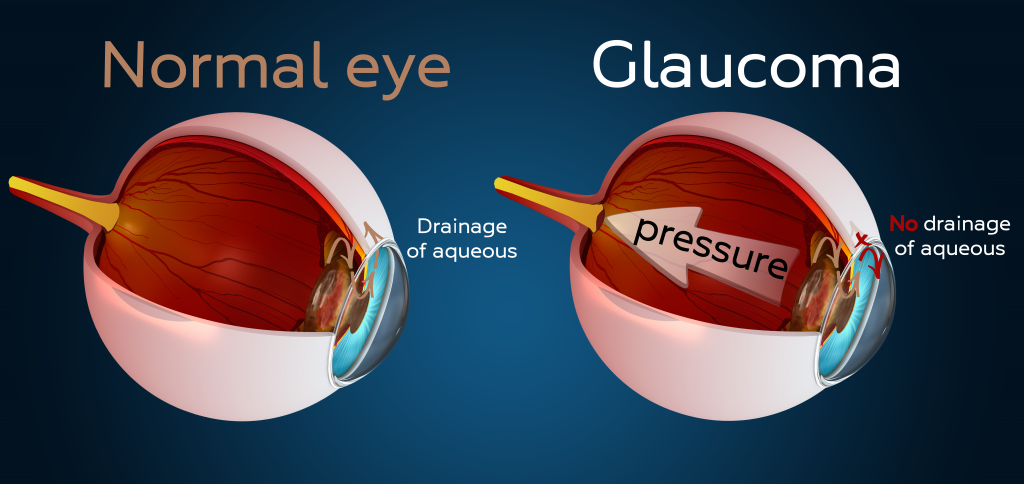
Your eye constantly makes aqueous. It is a clear fluid in the front part of your eye. It is responsible for keeping the shape of your eye correct and nourishing the eye. It is not the same as tears. New aqueous is constantly produced in your eye and the same amount should drain out through the drainage angle. This keeps the pressure (intraocular pressure IOP) in your eye stable. If the drainage angle is not working correctly, fluid builds up and pressure inside the eye increases. This damages the optic nerve that is responsible for sending light signals to your brain so you can see.
This nerve consists of hundreds of thousands of nerve fibers that are killed one by one due to the high pressure. You will develop blind spots in your vision. Amazingly your brain fills in these blind spots and although some detail will be missing you might not suspect anything until you have lost a great part of your vision. If all of the fibers die, you will be blind. Managing the pressure should however spare your nerve fibers and prevent blindness.
Two types of glaucoma
Open-angle glaucoma:
Open-angle glaucoma is the most common form of the disease. The drainage angle formed by the cornea and iris remains open, but the trabecular meshwork is partially blocked. This causes pressure in the eye to gradually increase. This pressure damages the optic nerve. It happens so slowly that you may lose vision before you’re even aware of a problem.
-
Patchy blind spots in your side (peripheral) or central vision
-
Tunnel vision in the advanced stages
Acute angle-closure glaucoma or closed-angle glaucoma or narrow-angle glaucoma:
This type of glaucoma happens when someone’s iris (the coloured part of the eye) is very close to the drainage angle in his or her eye. The iris can block the drainage angle. You can think of it like a piece of plastic over a sink drain. The drainage angle gets completely blocked and eye pressure rises very quickly. This is an emergency and you should call your ophthalmologist immediately or you might go blind.
The signs of an acute angle-closure glaucoma attack:
- Sudden blurry vision
- Severe eye pain
- Headache
- Nausea & vomiting
- Seeing rainbow-coloured halos around lights
Angle-closure glaucoma can also develop slowly. This is called chronic angle-closure glaucoma. You have no symptoms at first. You only realize you have it when the damage is severe or you have an acute attack. Angle-closure glaucoma can cause blindness if not treated immediately.
Diagnosing glaucoma
It is essential to check both the pressure in your eye and examine the optic nerve to screen for glaucoma.
Your doctor will:
- Measure your eye pressure (IOP)
- Inspect your eye’s drainage angle
- Test your peripheral (side) vision Visual Field
- Examine your optic nerve for damage and or take a picture. As well as do a computer measurement of your optic nerve OCT.
- Measure the thickness of cornea


How high is your risk for glaucoma?
Your risk is higher if you:
- are older than 40
- have family members with glaucoma
- are of African or Hispanic descent
- have high eye pressure
- are far-sighted or near-sighted
- had a previous eye injury
- have corneas that are thin in the center
- have thinning of the optic nerve
- have diabetes, migraines, poor blood circulation or other health problems affecting the whole body
If you have more than one of these risk factors you have an even higher risk of glaucoma.
Treating glaucoma
Damage due to glaucoma cannot be reversed. It is permanent. Further damage can however be prevented with medicine and surgery. Treatment options include medication, laser surgery and hospital surgery.
Glaucoma is usually controlled with eye drops
- The eye drops lower eye pressure. They either reduce aqueous fluid production or improve drainage at the drainage angle. The aim is to prevent further vision loss. All medications can have side effects. Some drugs can cause problems when combined with other medications. Tell your doctor about all the medicine you take regularly. Never change or stop taking your glaucoma medications without talking to your eye doctor. Also make sure that you do not run out of your medication.
Glaucoma surgery in hospital creates a new drainage channel for the aqueous to leave the eye
- Trabeculectomy. This is where your eye surgeon creates a tiny flap in the sclera (white part of your eye). A bubble (like a pocket) is also formed in the conjunctiva called a filtration bleb. It is usually hidden under the upper eyelid and cannot be seen. Aqueous humor will be able to drain out of the eye through the flap and into the bleb. In the bleb, the fluid is absorbed by tissue around your eye, lowering eye pressure.
- Glaucoma drainage devices. Your ophthalmologist may implant a tiny drainage tube in your eye. It sends the fluid to a collection area. Your eye surgeon creates collection area (reservoir) beneath the conjunctiva that covers the white part of your eye. The fluid is absorbed into nearby blood vessels.
- Minimally-invasive glaucoma surgery (MIGS) can be done at the time of cataract surgery for patients with mild to moderate open angle glaucoma. It requires no additional incisions other than those needed for cataract surgery itself. The device creates a bypass through the blockage site. Patient recovery time is usually rapid. Clinical studies show that most patients experience a reduction in IOP and a reduction in reliance on glaucoma medication.
Your role in the treatment
Treating glaucoma successfully is a team effort between you and your doctor. Your eye doctor will prescribe your glaucoma treatment. It is up to you to follow your doctor’s instructions and use your eye drops. Once you are taking medications for glaucoma, your ophthalmologist will want to see you regularly. You can expect to visit your ophthalmologist about every 3-6 months.